- Home
- China
- World
- Europe
- Politics
- Business
- Opinions
- Tech & Sci
- Culture
- Sports
- Travel
- Nature
- Picture
- Video
- Live
- TV
- Specials

Share

Copied

A Belgian medical worker does a COVID-19 test on staff at an elderly residence in Brussels, Belgium. Kenzo TRIBOUILLARD / AFP
Around 10,000 extra people are dying each week in Europe, according to the latest information from The University of Oxford's Centre for Evidence-Based Medicine (CEBM) released on Monday.
Unsurprisingly, COVID-19 is driving the spike in deaths – primarily among the over-65s, who account for nearly 80 percent of total fatalities.
Each week, the CEBM publishes Europe's mortality rate. Since the pandemic began to increase that rate significantly, it started to look more closely at COVID-19's effect on the continent's death rate to help scientists understand more about the coronavirus, how many people are infected and how deadly it is, which the group calls its "case fatality rate."
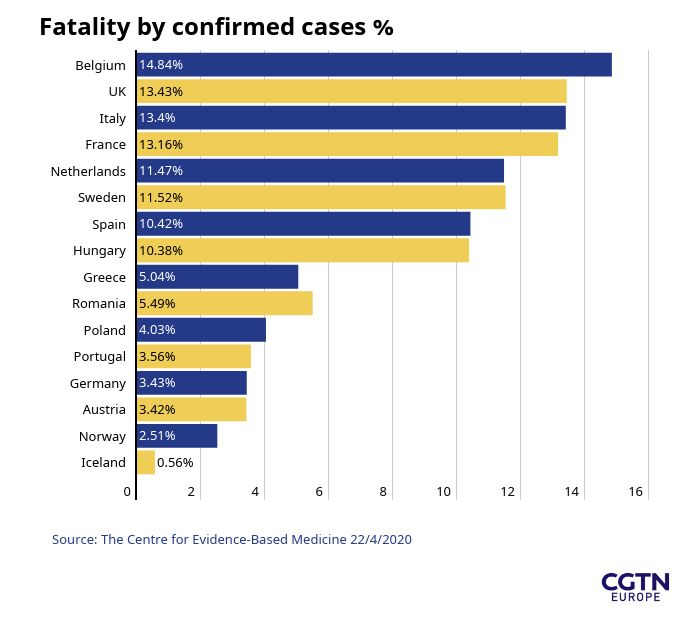
Lockdowns in Spain, Italy and elsewhere are helping to slow the spread of the coronavirus and aggregate deaths are starting to plateau at a level more in line with the seasonal average. Some countries, however, have case fatality rates as high as 15 percent. In others, such as Iceland, it's just 0.51 percent.
Understanding why there is such a disparity holds the key to knowing more about this silent killer.
Measuring fatalities
Different types of testing mean the number of recorded cases of infection in each country are not comparable, so focusing on how many people die from COVID-19 is the most accurate tool scientists have to understand more about it.
"Mortality does not lie, it is not open to alternative explanations, something which bedevils observational data," note Tom Jefferson and Carl Heneghan, the authors of the latest CEBM report.
Nevertheless, even the number of deaths recorded from the coronavirus can vary because those that occur outside hospitals can't always be attributed to the virus. The UK, for instance, does not include the large number of deaths that happen in care homes for the elderly in its figures, although Belgium does, even including deaths suspected, but not confirmed, to be linked to coronavirus.
It can also be difficult to determine whether a patient who dies after testing positive for COVID-19 has died directly as a result of contracting the virus or from another cause, especially as many of the most serious cases involve patients with pre-existing health problems. Most countries, such as Germany, count any death in which coronavirus was present among their numbers for the disease.
Cases and fatality rates
Measuring the percentage of those suffering COVID-19 who succumb to the disease is even more complicated, because of the challenges in identifying the total number of people infected.
Selection bias may mean that only those presenting severe symptoms receive a test, which in turn will push up a nation's case fatality rate. Until recently, this had been the case in the UK, where only patients spending the night in hospital would receive a test.
When Italy changed its policy on 25 February, limiting testing to patients showing severe symptoms, its COVID-19 mortality rate nearly doubled to 7.2 percent within a month because those with milder symptoms were no longer being tested.
The CEBM's findings show that significantly more people are infected than have been tested. Many are asymptomatic: other recent studies indicate that more than 50 percent of carriers display no symptoms whatsoever.
Increased testing is key. In both South Korea and the Gangelt area of Germany, mass testing programs on random samples of the population brought many positive tests on people showing no symptoms.
Antibody testing could hold the key to infection fatality rate data being accurate. Unlike a regular test, which deals with only whether the virus is in the host at that point, it can determine if someone has been infected at some point and possibly has developed immunity.