- Home
- China
- World
- Europe
- Politics
- Business
- Opinions
- Tech & Sci
- Culture
- Sports
- Travel
- Nature
- Picture
- Video
- Live
- TV
- Specials

Share

Copied

Being older, having a pre-existing condition and quite possibly being male may all make COVID-19 sufferers at great risk of death. /Science Photo Library/Getty Creative
First, a caveat: nobody yet knows the definitive answers to these questions. The COVID-19 coronavirus is new, the world's leading experts admit there is much they still have to learn, and the disease will have to run its course before we can have complete figures.
Working from the data available, scientists have gone as far as to say it is likely that the mortality rate may end up being lower than 1 percent, albeit increasing to between 8 and 9 percent for those over 80 years old. That would mean more than a 90 percent recovery rate even for octogenarians.
For comparison, the fatality rate of seasonal flu averages 0.1 percent, but of a much bigger number – a total so difficult to estimate that the U.S.-based Center for Disease Control suggests influenza causes "between nine million and 45 million illnesses" annually in the U.S. alone, while the World Health Organization (WHO) blames seasonal flu for "about 290,000 to 650,000 respiratory deaths" globally per year.

There is a vaccine for seasonal flu; there isn't one yet for COVID-19. /JurgaR/Getty Creative
The time-lapse problem
One important thing to consider is the lag between reporting and death. A WHO report in late February noted that the time between symptom onset and fatality ranged between two and eight weeks; even at its shortest, with the rapidly rising number of cases, there will be a delay, which could significantly distort the mortality rate.
On Monday 9 March, the WHO reported an ongoing total of 3,809 deaths from 109,577 confirmed cases, which on bare numbers – dividing the number of deaths by the number of cases – represents a 3.47 percent death rate.
Two weeks previously, those numbers were 2,618 deaths from 79,331 cases; that represents 3.3 percent fatality, but more statistically importantly it means that in the past two weeks alone there have been another 30,246 cases, each of which must run its course before scientists can claim an accurate mortality rate.
But where might the spread be by then? Eight weeks ago – on 13 January, the day the first case was confirmed outside China – the WHO hadn't even started compiling its regular statistical updates, but there had been just one death from around 42 cases. If two weeks is a long time in this outbreak, eight weeks makes a world of difference.

A doctor checks the body temperature of a man coming into India at the border with Bangladesh. /Diptendu Dutta/AFP
Fluctuations through reporting
Even with that epidemiological asterisk, scientists have been estimating the mortality rate. After preliminary suggestions that it was around 2 percent. In early March, the WHO suggested it was 3.4 percent of reported cases.
However, the WHO says about 80 percent of those with the infection only experience mild symptoms; they are therefore less likely to be tested – and to be counted among the case numbers. As diagnostic capacity increases, we will get a truer sense of the actual number of infections – which should drive the mortality rate down.
This is more than just a statistical hunch. In some countries where testing has been more widespread, mortality rates appear to be lower. South Korea, for example, has carried out tests on more than 1,100 people for every one million; its official mortality rate has been calculated at around 0.68 percent.
On the other hand, in the U.S., where initially limited testing capacity prompted a strategy of focusing on more severe symptoms, the mortality rate rose above 5 percent. That may well come down significantly as more diagnostic kits become available.
However, Italy is an outlier. Despite aggressive testing, the country's mortality rate currently stands at around 5 percent. That doesn't necessarily mean the virus is more deadly there than in other countries and regions: Italy's own testing strategy, for example, could explain the higher percentage and this figure may even out over time.

A masked tourist walks past the closed and near-deserted Coliseum in Rome. /Alberto Pizzoli/AFP
Underlying demographics
It is also possible that demographics play a role, though. The elderly seem to be more vulnerable, and Italy's population is one of the oldest in the world. Many other European countries are also ageing societies, which is worrying health experts.
Other vulnerable groups are those with underlying health issues. Again, it is important to stress that no figures are complete at this stage. Nonetheless, early reports from the outbreak suggest around 40 percent of people who were hospitalized with coronavirus had a heart condition.
The New England Journal of Medicine looked at 1,099 cases from the outbreak epicenter of Wuhan as of 29 January and found that those with diabetes, higher blood pressure, heart disease, chronic obstructive pulmonary disease, hepatitis B, cancer and renal disease were more likely to get sicker. (The report is here, with details at the bottom of Table 1.)
Experts say conditions that people will be more vulnerable to stronger symptoms if they conditions which lower the strength of the body's immune system or hamper the workings of the lungs. That includes asthma, which the WHO says is "most common chronic disease among children worldwide," afflicting "around 235 million people."

Asthma is the most common chronic disease among children. Karl Tapales/Getty Creative
Some preliminary numbers
It's difficult to make a clear assessment of vulnerability. Drilling down into the statistics is tricky: not only is COVID-19 a fast-moving, widespread outbreak, but not every health authority collects or releases the same amount of detail on case sufferers.
However, on 29 February Worldometers.info analyzed the best data available from two major sources: the 28 February report of the WHO-China Joint Mission based on 55,924 laboratory-corroborated cases (which Worldometers calls "confirmed cases") and a 17 February paper by the Chinese CCDC based on 72,314 confirmed, suspected, and asymptomatic cases in China ("all cases").
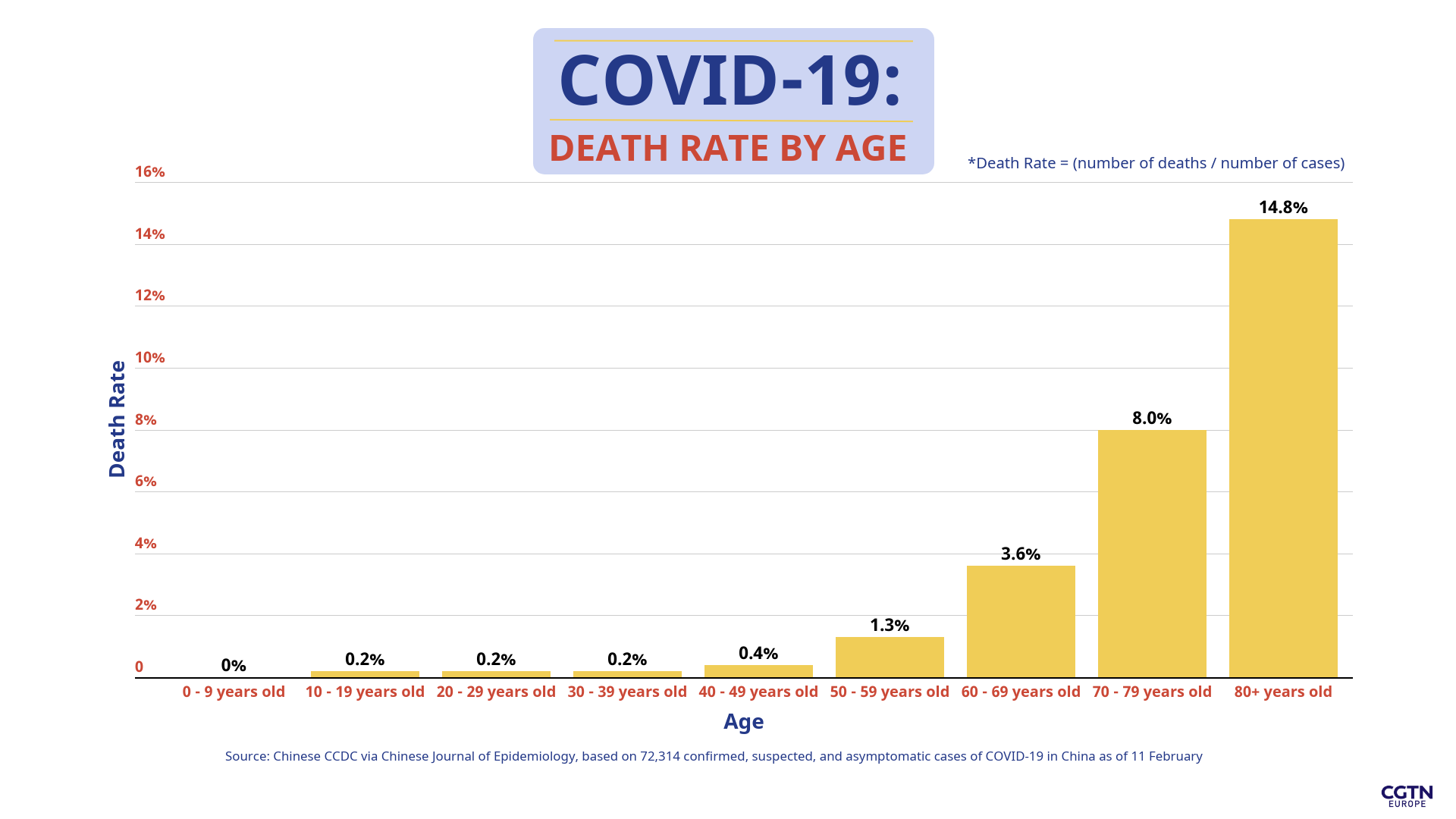
The CCDC "all cases" report suggested a strong correlation between age and COVID-19 mortality. The death rate for each decade under 50 was well below 1 percent, rising to 1.3 percent for victims in their 50s, through 3.6 percent for 60-somethings and 8 percent for those in their 70s, to 14.8 percent for those aged 80 or above.
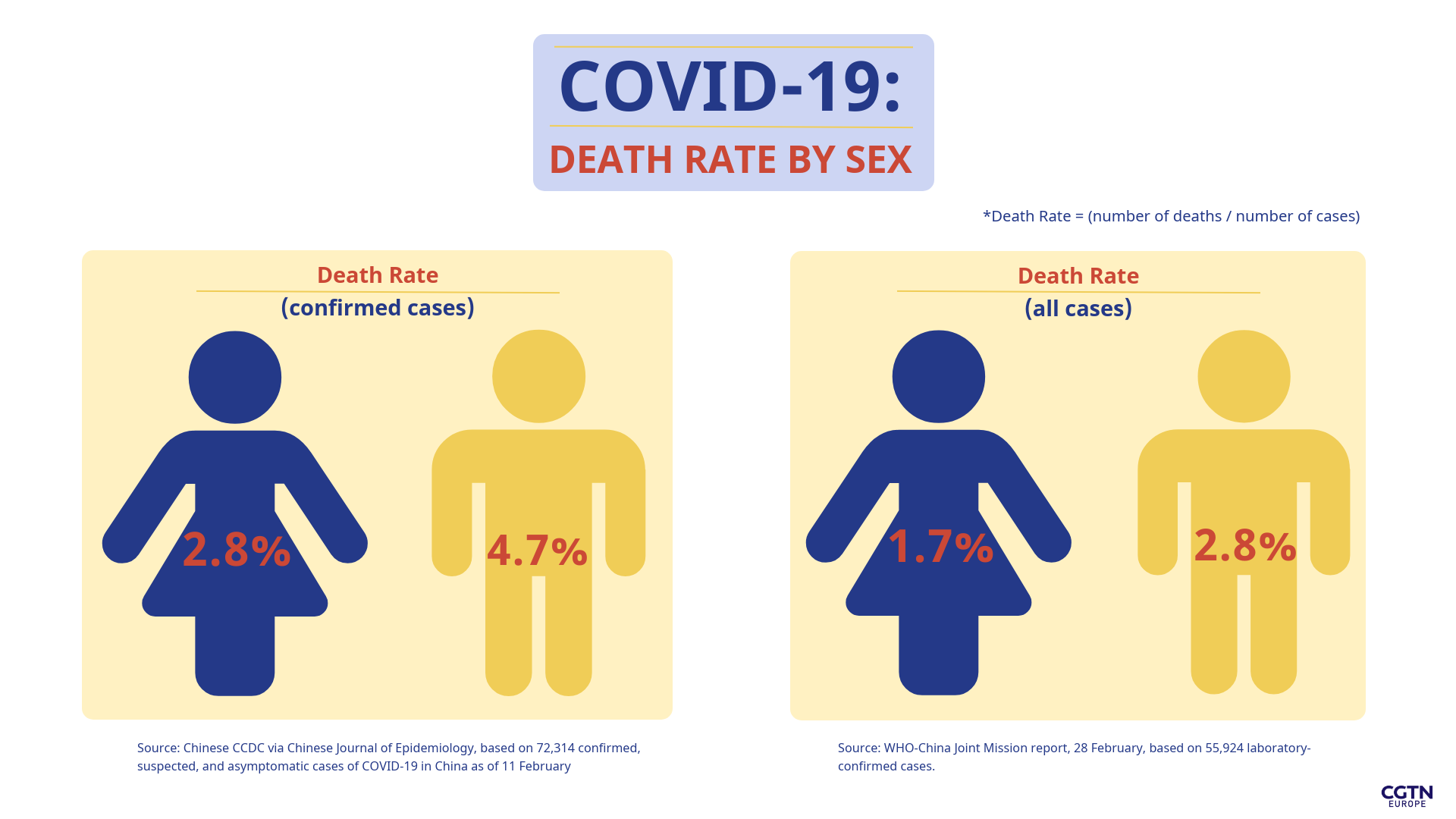
Analyzing by sex, Worldometers could call upon both studies, each of which showed a pronounced rise in mortality for men compared with women. The "all cases" CCDC study reported 2.8 percent of male cases and 1.7 percent of female victims dying, while the Joint Mission "confirmed cases" study reported 4.7 percent for men and 2.8 percent for women. It has been suggested that this may be because smoking in China is much more prevalent among men.
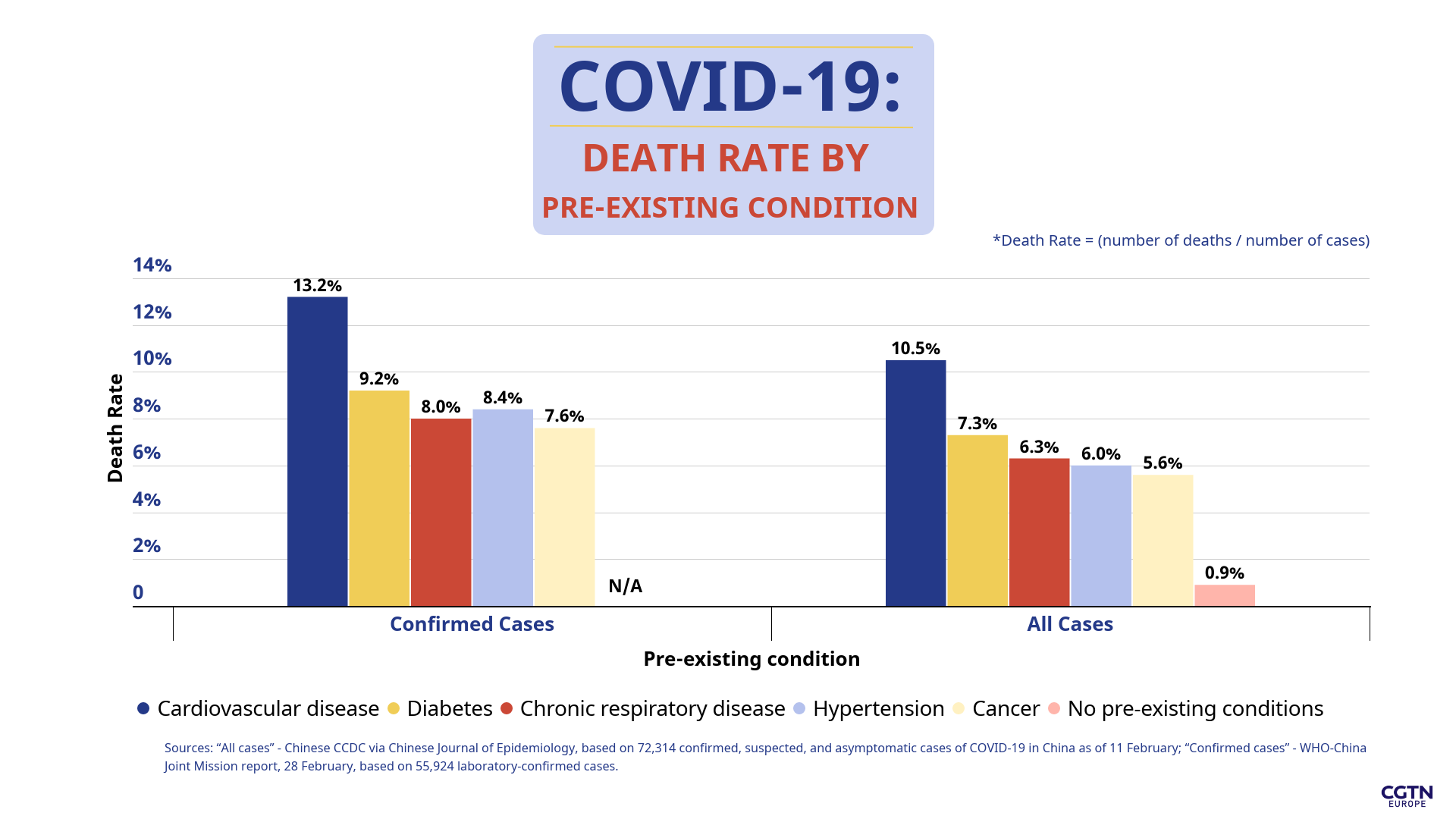
Finally, pre-existing conditions. Again, both reports can be used as source data and, while statisticians must always be careful not to confuse correlation with causation, there are definitely strong links between some pre-existing conditions and a higher mortality rate.
Worst of all is cardiovascular disease, with a 13.2 percent mortality rate among confirmed cases. Diabetes (9.2 percent), hypertension (8.4 percent), chronic respiratory disease (8 percent) and cancer (7.6 percent) also correlate with higher mortality rates – broadly matched, if at a slightly lower level, by the deeper but earlier "all cases" data.
So, it seems there are general themes to be pulled out of these figures, if with some uncertainty until those February figures are corroborated: men are more at risk, age plays a notable part and so do some pre-existing conditions.
However, perhaps we should also heed the words of the WHO director-general, Tedros Adhanom Ghebreyesus, who wants us to keep it simple. "The death rate from this outbreak is high. We shouldn't categorize by young or senior," he told reporters on Monday.
"Of course, to understand the epidemiology, it's fine to do that," he continued. "But for action, I think every life matters. This is a moral decay if we try to categorize it that way: a moral decay of society."